The first session is a juggle: empathy, safety, and structure—while your brain is also triaging risk and formulating care. Early in their careers, many clinicians over-collect history and under-document clinical reasoning. Insurance audits usually cure that habit quickly.
Intake notes set the tone for treatment. Done well, they capture just enough history to be safe and smart, highlight the working diagnosis, and map next steps—without drowning in biography.
This guide shows you how to write therapy intake notes that are clear, defensible, and genuinely helpful for session two. We’ll connect your intake with your ongoing progress notes, session-level SOAP notes, and your formal treatment plan.
What Therapy Intake Notes Are (and Aren’t)
Intake notes document the first clinical encounter. They capture referral context, present concerns, relevant history, mental status, initial risk picture, a working diagnosis (if indicated), and an initial plan. They are not an autobiography. Your goal is to record the information that will shape care from visit two onward.
- Prioritize safety and direction: Record risks, protective factors, and immediate next steps.
- Decide what matters now: Include history that changes your formulation or plan; skip the rest.
- Write for continuity: If another clinician covered your next session, they should be able to proceed confidently based on this note.
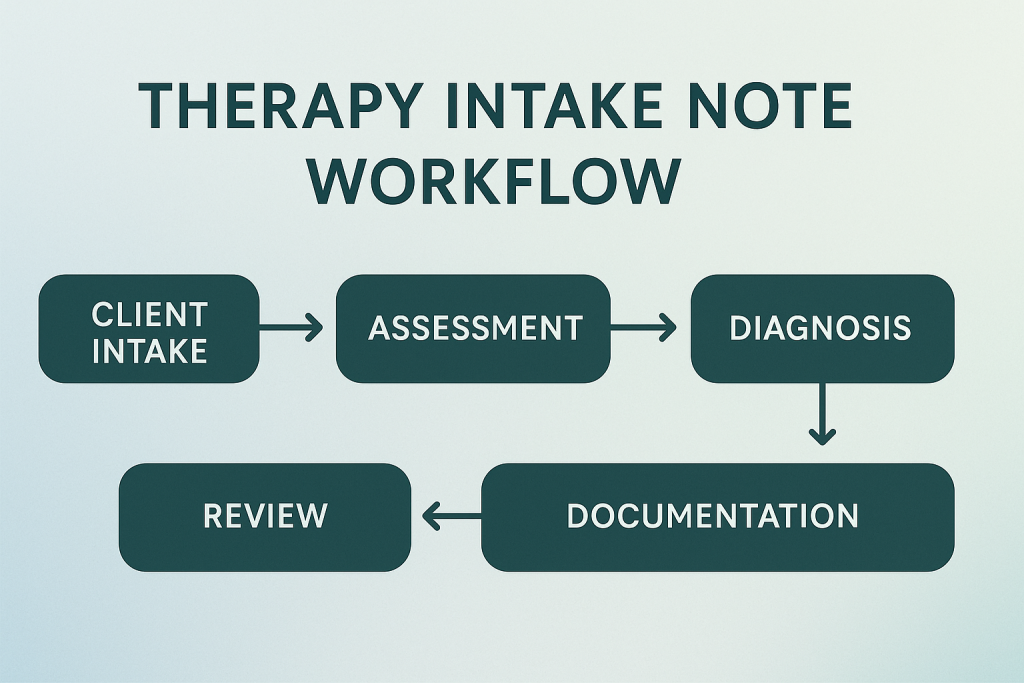
The Intake Note Workflow
A successful intake flows from data collection to clinical formulation, ending with a concrete treatment direction.
A Simple, Readable Structure
You can use SOAP or DAP formats if you prefer, but regardless of the acronym, stick to this clear narrative outline. Make each line earn its spot:
Session Details & Presenting Concerns
Session details: Date/time, modality (in-person/telehealth), duration, who participated.
Referral context: Why is the client seeking therapy now? What is the most impairing symptom?
History, Screeners, & Risk
Relevant history: Brief behavioral health history, medical, meds, and family/social highlights that actively change care.
Screeners & risk: Include PHQ-9/GAD-7 scores if used. Explicitly document suicidality, self-harm, harm to others, substance use, and the client's protective factors.
Clinical Assessment & Formulation
Mental Status Exam (MSE): Appearance, behavior, speech, mood/affect, thought process/content, orientation, insight/judgment.
Formulation: A concise synthesis linking symptoms, context, and mechanisms keeping the problem going.
Diagnosis & Initial Plan
Working diagnosis: Note the ICD-10 code alongside a one-sentence clinical rationale.
Initial plan: Note the frequency of future visits, modalities planned, homework assigned, referrals, safety supervision protocols, and the next steps toward building a formal treatment plan.
Intake Note Examples
These examples are intentionally concise. Adjust the depth to your specific clinic setting and payer requirements.
📝 Example 1: Individual Therapy (Anxiety)
💊 Example 2: Med Management (Depression)
💬 Example 3: Couples Therapy Intake
Time-Savers & Common Pitfalls
Design Your Intake Script
A short, standardized sequence for risk, impairments, and goals keeps the interview moving and ensures you don't miss vital compliance checkpoints for your CPT 99203 billing.
Oversharing History
If a historical detail does not change your formulation or treatment plan, leave it out. Long, rambling narratives that don't affect care simply increase your liability and waste administrative time.
Use Scalable Measures
Use the exact same measures (PHQ-9, GAD-7, or functional markers like sleep/attendance) in your intake that you plan to trend later. This allows you to objectively prove medical necessity to auditors during later chart reviews.
Stop Guessing on Compliance.
Start Getting Paid.
- Professional Medical Coding & Billing
- Denial Management & Appeals
- FREE Insurance Credentialing
- FREE TherapyDial Profile Listing
We verify your codes, submit your claims, and fight for your revenue.
HIPAA Compliant & Expertly Managed.
Master Your Clinical Documentation
Ensure your practice remains compliant from intake to discharge with our related hubs:
Clinical Documentation
Diagnostic Coding Mastery
Frequently Asked Questions About Intake Notes
Often 1–2 pages. Focus on present concerns, risk, MSE, formulation, working diagnosis, and an initial plan. It does not need to be an exhaustive biography.
A "working diagnosis" is helpful if supported by symptoms and functional impairment. This is often required to bill the initial session to insurance. It can be revised in future sessions as more data accumulates.
Direct quotes regarding suicidality/homicide, timing, intent, means, protective factors, and specific actions taken (e.g., safety plan created, supervision level established).
Document what was completed, specifically noting that immediate risks were addressed, and outline the plan to finish the remaining assessment items during the next visit.