How to Write a Mental Health Treatment Plan
Writing a solid treatment plan is one of the most meaningful parts of therapy—it transforms insight into direction. Here’s how to do it well, efficiently, and confidently.
Writing progress notes is one thing. But crafting a treatment plan? That’s where your clinical intuition meets structure.
I still remember my first week out of grad school—sitting at my desk staring at a blank template, wondering, “How do I turn the client’s story into a plan?” Over time (and after many audits), I learned that a mental health treatment plan is less about filling boxes and more about charting a course. In this article, we’ll explore exactly how to write a mental health treatment plan that’s compliant, collaborative, and clinically meaningful.
What is a mental health treatment plan?
A mental health treatment plan is a structured document outlining a client’s presenting issues, therapeutic goals, interventions, and progress measures. It’s both a roadmap for therapy and a communication tool for care coordination. When you learn how to write a mental health treatment plan well, you build a bridge between diagnosis and recovery—turning “what’s wrong” into “what’s next.”
Why treatment plans matter — compliance, clarity, and care
For insurance and compliance, treatment plans demonstrate medical necessity—showing that care is active, structured, and goal-oriented. For clients, they bring transparency: a shared understanding of what therapy aims to achieve.
Clinical Perspective: I often tell new clinicians, "Your treatment plan is like a map. It’s not about controlling the journey, but it keeps you from getting lost."
Core elements of a treatment plan
Client Information
Demographics, diagnosis (e.g., ICD-10 F41.1), and relevant history.
Presenting Problems
The client’s main concerns, symptoms, and functional impairments.
Goals & Objectives
Broad, meaningful outcomes paired with specific, measurable steps.
Interventions & Progress
Specific therapeutic methods used and how improvement is tracked over a scheduled review timeline.
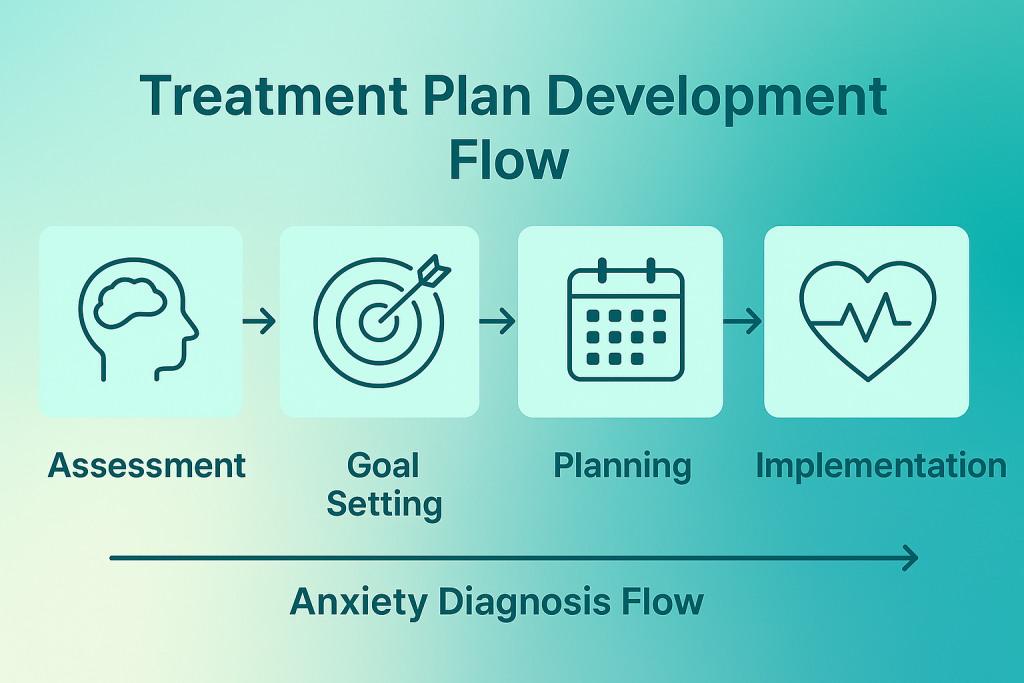
How to write a mental health treatment plan — step-by-step
Here’s a proven framework I use and teach to new therapists. Think of it like the clinical cousin of SOAP notes—structured, flexible, and built for clarity.
1. Start with a comprehensive assessment
Gather intake data, mental status, risk assessment, and relevant history. This initial intake informs every downstream decision.
2. Define the presenting problems
Start with the client’s language, then translate into clinical terms. Precision here reduces ambiguity later and supports medical necessity.
3. Create meaningful, measurable goals
Goals should connect directly to problems and be trackable (e.g., “Reduce daily anxiety from 8/10 to 4/10 in 8 weeks”).
4. Write SMART objectives
Specific, Measurable, Achievable, Relevant, Time-bound. Keep them realistic and behaviorally written.
5. Choose interventions and modalities
Specify your methods and cadence (e.g., CBT weekly + mindfulness homework). This shows an active, intentional plan.
6. Determine how progress will be measured
Use standardized tools (PHQ-9, GAD-7), symptom logs, or functional metrics. Document baselines and targets.
7. Plan regular reviews
Re-evaluate every 30–60 days; adjust goals and interventions as needed. Document rationale for plan changes.
Example treatment plan
Tips, insights, and key takeaways
- Co-create with clients; shared ownership improves clinical adherence and trust.
- Write clearly: Write as if another clinician will take over tomorrow—clarity beats shorthand.
- Use standardized scales (PHQ-9, GAD-7) to show objective change, which insurers expect.
- Document cultural factors that shape goals and engagement.
- Set calendar reminders to revisit plans monthly to avoid compliance gaps.
Stop Stressing Over Documentation.
Start Getting Paid.
- Professional Medical Coding & Billing
- Audit-Proof Documentation Templates
- FREE Insurance Credentialing
- FREE TherapyDial Profile Listing
We verify your codes, submit your claims, and fight for your revenue.
HIPAA Compliant & Expertly Managed.
Frequently asked questions
Typically 1–2 pages—concise yet comprehensive, with measurable goals and clear interventions. It should be long enough to cover medical necessity but short enough to be readable.
Usually every 30–60 days or when major clinical changes occur. Always document the rationale for any updates or goal changes in your notes.
Yes. Collaboration improves engagement and clarity. Many modern EHRs support client portals that allow for secure transparency.
Simply revise the goals and objectives and note the reason for the pivot. Treatment plans are living documents meant to adapt to the client's journey.
Yes. Strengths-based planning supports motivation and resilience and is highly favored in modern clinical documentation standards.
TherapyDial Editorial Team
Clinical Documentation & Compliance Experts
This guide was developed and reviewed by licensed therapists and compliance officers to ensure accuracy, clarity, and adherence to 2026 insurance and state board standards.