What Are Body-Focused Repetitive Behaviors?
Body-Focused Repetitive Behaviors (BFRBs) are a group of behaviors where individuals repeatedly damage or manipulate their own bodies, often as a response to emotional triggers or without even realizing they’re doing it. These aren’t just “bad habits”—they’re complex psychological disorders that can significantly impact a person’s quality of life.
Common BFRBs include pulling out hair (trichotillomania), picking at skin (dermatillomania or excoriation disorder), biting nails, or chewing the inside of the cheeks. While many people occasionally engage in these actions, those with BFRBs do them compulsively and often feel unable to stop, even when it leads to visible damage, pain, or distress.
What makes BFRBs especially difficult is how they sneak into everyday life. They can happen while watching TV, sitting in class, working at a desk, or lying in bed. They’re often subconscious—automatic behaviors that provide temporary relief, but long-term guilt, shame, and even physical harm.
Why BFRBs Are Often Misunderstood
Because many BFRBs look like harmless habits—like nail biting or fidgeting—they’re often brushed off by others as quirks or nervous tics. But for those living with them, they’re anything but harmless. They can cause bleeding, infection, bald patches, scars, and intense emotional suffering.
Society doesn’t always make room for visible signs of mental distress. People with BFRBs often go to great lengths to hide the evidence—wearing hats to cover hair loss, using makeup to conceal scabs, or avoiding social situations out of embarrassment.
That misunderstanding and stigma keep many people from seeking help. BFRBs are underdiagnosed, underreported, and under-discussed—even though they affect millions globally. The good news? With better awareness, compassionate care, and science-backed treatment, healing and management are absolutely possible.
Types of BFRBs
Hair Pulling (Trichotillomania)
Trichotillomania is one of the most well-known BFRBs. It involves recurrent, irresistible urges to pull out hair from the scalp, eyebrows, eyelashes, or other parts of the body. For some, it’s about removing individual hairs that “feel wrong.” For others, it’s driven by anxiety, boredom, or an intense need for control.
Hair pulling can be ritualistic—examining the root, running hair through the fingers, or even ingesting it (a condition known as trichophagia). Over time, this leads to noticeable hair loss, bald spots, and emotional pain.
People with trich often report a feeling of tension before pulling and a sense of relief afterward—followed by guilt or frustration. It’s a cycle that’s hard to break without support.
Skin Picking (Dermatillomania or Excoriation Disorder)
Dermatillomania involves compulsively picking at skin, often resulting in open wounds, scabs, infections, or scarring. Some people pick at perceived imperfections, while others focus on real blemishes like acne or rough patches.
Like trich, skin picking can be both conscious and unconscious. It may happen during stressful moments, but also in times of relaxation. Many sufferers don’t even realize how much time they spend picking until the physical consequences show up.
The face, arms, and legs are common areas, but people may pick anywhere. The shame associated with visible wounds can lead to long sleeves in summer, avoiding mirrors, or withdrawing from loved ones.

Nail Biting and Cheek Biting
While nail biting (onychophagia) is often seen as a common childhood habit, in some cases it persists into adulthood and becomes compulsive. People may bite nails to the quick, chew cuticles, or gnaw at hangnails until they bleed.
Cheek biting (morsicatio buccarum) involves chewing the inside of the cheeks or lips. It can create sores, callouses, or chronic irritation—and is often paired with anxiety or periods of intense focus.
Both behaviors can interfere with daily life, cause pain, and lead to infection if left untreated.
Less Common BFRBs
Other BFRBs may include:
- Nose picking (rhinotillexomania)
- Lip biting or peeling
- Scab picking (secondary to wounds)
- Cuticle tearing
While these may sound less severe, they can be just as distressing. The common denominator is that these actions are compulsive, harmful, and difficult to control, often despite repeated attempts to stop.
Signs and Symptoms of BFRBs
Physical Signs
BFRBs often leave behind clear signs—especially when they become chronic. These may include:
- Bald patches or thinning hair
- Open sores, scabs, or scars
- Redness or swelling around fingernails or lips
- Chewed cheeks, dry lips, or missing cuticles
- Frequent bandage use or hiding affected areas with makeup or clothing
These physical signs can lead to secondary infections, permanent scarring, or long-term dermatological issues. That’s why early intervention is so crucial.
Emotional and Behavioral Patterns
Beyond the physical, BFRBs are deeply emotional. People often feel:
- Shame or guilt after engaging in the behavior
- Anxiety before, during, or after episodes
- Isolation or embarrassment, especially in public settings
- Relief or satisfaction during the act itself
- Frustration at not being able to stop, even with strong motivation
Behaviorally, you might notice:
- Long periods spent in front of mirrors or in the bathroom
- Pulling or picking during passive activities (TV, reading)
- Hiding the behavior from family or friends
- Creating rituals around the behavior
Many individuals live in silence, believing they’re the only ones doing this. But they’re far from alone.
Causes and Risk Factors
Genetic Predispositions
Research suggests that BFRBs may run in families. If a parent, sibling, or close relative has a BFRB or related condition like obsessive-compulsive disorder (OCD), anxiety, or tic disorders, the risk may be higher. While no single “BFRB gene” has been identified, there seems to be a hereditary component tied to impulse control and emotional regulation.
Twin studies also support the idea that BFRBs may have a genetic underpinning. In identical twins, if one twin has trichotillomania or dermatillomania, the other twin is more likely to have it as well, even when raised in different environments.
This doesn’t mean someone is “doomed” to develop a BFRB, but it helps explain why some people are more vulnerable—especially when combined with environmental stressors.
Emotional Triggers (Anxiety, Boredom, Stress)
Emotions play a huge role in BFRBs. Many people report that picking or pulling helps relieve tension, soothe boredom, or give a sense of control when life feels overwhelming. These behaviors often serve as a coping mechanism—a way to self-soothe when other strategies aren’t available.
Common emotional triggers include:
- Stress or conflict (school, work, relationships)
- Anxiety or overstimulation
- Depression or low energy states
- Boredom or long periods of inactivity
- Perfectionism or obsessive thoughts
Unfortunately, the temporary relief from these behaviors reinforces them. The brain begins to associate picking or pulling with emotional comfort, making the habit harder to break.
Neurological and Psychological Factors
BFRBs are believed to involve dysregulation in the brain’s reward and habit-forming systems, particularly in the basal ganglia and prefrontal cortex. These areas control decision-making, impulse control, and reward processing.
This is why people with BFRBs often describe a sense of being on “autopilot.” They may not even be aware they’re engaging in the behavior until it’s already done—or until pain or damage stops them.
There are also links between BFRBs and conditions such as:
- OCD (Obsessive-Compulsive Disorder)
- ADHD (Attention Deficit Hyperactivity Disorder)
- Anxiety disorders
- Autism Spectrum Disorder
Each of these shares traits like sensory sensitivity, perfectionism, or difficulty with emotional regulation—all of which can feed into BFRB patterns.
How BFRBs Affect Daily Life
Physical Health Risks
Repeated pulling, picking, or biting can cause serious physical issues:
- Infections from open wounds or torn skin
- Hair loss or permanent damage to follicles
- Scarring and tissue damage
- Dental issues from chronic biting
- Bleeding or pain, sometimes leading to hospital visits
In severe cases, complications like cellulitis (a skin infection), trichobezoars (hairballs from ingesting hair), or disfigurement can occur.
Emotional and Social Consequences
BFRBs aren’t just physically painful—they take a major toll on emotional health:
- Shame and self-blame after episodes
- Fear of judgment, leading to secrecy and isolation
- Low self-esteem, especially if appearance is affected
- Depression due to chronic struggle and lack of control
Many people with BFRBs avoid dating, social events, or even public places because they’re afraid of being noticed or misunderstood. This isolation can deepen the emotional pain, creating a feedback loop that worsens the behavior.
Impact on Self-Esteem and Mental Health
Perhaps the most heartbreaking impact of BFRBs is on self-worth. Constant urges, daily damage, and the inability to stop can make people feel weak, broken, or “disgusting.” This often leads to:
- Negative self-talk
- Body image issues
- Withdrawal from hobbies, school, or work
- Increased risk of depression and anxiety
The psychological burden is heavy. But with support, understanding, and appropriate treatment, people can reclaim their confidence and reduce or even eliminate these behaviors.
Diagnosis and When to Seek Help
Recognizing the Disorder Beyond “Bad Habits”
One of the biggest barriers to diagnosis is the belief that BFRBs are just nervous habits. But true BFRBs are chronic, compulsive, and emotionally distressing. They interfere with life, cause real harm, and persist despite efforts to stop.
You might need help if:
- The behavior is causing physical damage
- You feel anxious, ashamed, or out of control
- You’ve tried to stop many times but can’t
- It’s affecting your school, work, or relationships
Recognizing that your behavior is part of a diagnosable, treatable condition—not just a quirk—is a powerful first step.
How Mental Health Professionals Diagnose BFRBs
BFRBs are classified in the DSM-5 under “Obsessive-Compulsive and Related Disorders.” Diagnosis usually involves:
- A detailed history of behaviors and triggers
- Assessment of frequency, intensity, and emotional impact
- Evaluation of any coexisting mental health conditions
A psychologist, psychiatrist, or licensed therapist familiar with BFRBs can offer an accurate diagnosis and guide treatment planning. There’s no shame in asking for help—it’s the beginning of healing.
Treatment Options for BFRBs
Cognitive Behavioral Therapy (CBT)
CBT is one of the most effective therapies for BFRBs. It helps individuals identify negative thought patterns that fuel the behavior and replace them with healthier coping strategies. In the context of BFRBs, CBT often includes learning how to interrupt the automatic cycle of picking, pulling, or biting.
For example, someone might believe, “I have to get this bump off my skin or I won’t be able to focus.” CBT helps challenge that belief and replace it with something more constructive: “My urge is valid, but I can choose a healthier action.”
Over time, CBT can reduce both the frequency and intensity of the urges by teaching skills like:
- Mindfulness
- Distress tolerance
- Emotional regulation
- Cognitive restructuring
Habit Reversal Training (HRT)
HRT is a specific, targeted behavioral therapy designed to stop repetitive behaviors by introducing new, competing ones. It works in three main steps:
- Awareness Training – Recognizing when, where, and why the behavior happens.
- Competing Response Training – Replacing the behavior with something physically incompatible, like clenching a fist instead of picking.
- Social Support – Enlisting trusted people to reinforce progress and help with accountability.
HRT has shown high success rates in clinical trials and is often the first line of treatment for disorders like trichotillomania and dermatillomania.
It can be used alongside CBT, and many therapists now integrate the two approaches for stronger results.
Medications and Their Role
While medication isn’t a cure for BFRBs, it can help manage coexisting conditions like anxiety, depression, or OCD that often fuel the behaviors. Common prescriptions include:
- SSRIs (like fluoxetine or sertraline) – to reduce obsessive thoughts and anxiety
- N-acetylcysteine (NAC) – a supplement that may reduce urges in some people
- Antipsychotics (in rare, severe cases)
Medication is most effective when combined with therapy. It can reduce the urge to pick or pull, but doesn’t teach new behaviors or skills on its own.
Coping Strategies and Daily Management

Using Fidget Tools and Substitutes
Fidget tools are lifesavers for many people with BFRBs. They provide safe, sensory stimulation that satisfies the need to touch, squeeze, scratch, or pull—without causing harm.
Popular tools include:
- Fidget cubes and spinners
- Putty or slime
- Textured fabric swatches
- Worry stones or smooth rocks
- Hairbrushes with varied textures
- Chewelry (safe chewable jewelry for oral BFRBs)
These can be carried in a pocket, purse, or desk drawer and used anytime the urge arises. The key is to make them accessible and automatic, so your brain begins to choose them instead of defaulting to harmful behaviors.
Tracking Behaviors and Identifying Triggers
Self-awareness is critical. Use a journal or tracking app to log:
- Times of day when BFRBs happen
- Emotional states (stress, boredom, sadness)
- Locations (bed, desk, mirror, etc.)
- What triggered the urge
This helps reveal patterns—like picking during phone calls or pulling after arguments—which can guide interventions. Over time, tracking also shows progress and reminds you that even small wins matter.
Building a Support System
You don’t have to go through this alone. Talk to trusted friends, family members, or support groups about your BFRB. The more people who understand your struggle, the more safety you create around yourself.
Support can look like:
- Texting a friend when the urge hits
- Asking a roommate to help with fidget tool reminders
- Joining an online BFRB group or forum
- Seeing a therapist regularly
Isolation makes BFRBs worse. Connection helps you heal.
ASMR and Sensory Soothing for BFRBs
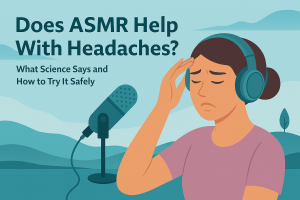
How ASMR Helps With Urge Reduction
ASMR (Autonomous Sensory Meridian Response) videos are growing in popularity as a calming tool—and they’re incredibly helpful for people with BFRBs. The soft sounds, slow visuals, and repetitive motions found in ASMR can soothe the nervous system and provide a sensory substitute during high-risk moments.
When you feel the urge to pick or pull, watching or listening to ASMR:
- Distracts your mind with gentle focus
- Mimics the comfort of sensory input
- Reduces anxiety, boredom, or overstimulation
It’s especially helpful in the evenings, when many BFRB behaviors intensify.
Top Triggers for Soothing Sensory Input
Try ASMR videos with:
- Hair brushing sounds
- Slow hand movements
- Soft whispering affirmations
- Light tapping and scratching
- Skincare roleplays (safe mirror time)
- Face tracing and “personal attention” content
These trigger calming brain waves, similar to meditation, and can gently guide your hands away from picking or pulling.
Many people create an “ASMR emergency playlist” they can reach for when the urge creeps in. It’s a digital comfort blanket—and it works.
Living With BFRBs: Real Stories
From Shame to Acceptance
One of the most powerful parts of recovery from BFRBs is realizing you’re not alone. For years, many individuals suffer in silence, afraid of being judged or misunderstood. But hearing stories from others who’ve faced the same struggles—and found ways to manage them—can be life-changing.
Take Kayla, for instance. She started pulling her eyelashes at age 10 and hid it for over a decade. After discovering the term “trichotillomania” online, she sought therapy and joined an online community. Now she shares her story openly and says, “The shame melted once I realized this was a disorder—not a flaw.”
Or Jamal, who picked his skin obsessively during high school and wore long sleeves year-round. After starting CBT and using fidget tools, he reports fewer episodes and more confidence in social settings.
These journeys show that while BFRBs are difficult, recovery is possible, and self-acceptance is the first, most vital step.
Success Stories and Recovery Journeys
Recovery doesn’t always mean “cure.” It often means:
- Less frequent urges
- More control over triggers
- Compassionate self-talk after a setback
- A life no longer defined by secrecy or shame
Whether through therapy, support groups, or tools like ASMR and HRT, many people have dramatically improved their relationship with their BFRB. They’ve gone from hiding to healing—and so can you.
Supporting Someone With a BFRB
What Not to Say or Do
If someone you love has a BFRB, your response matters. These behaviors may look like habits, but they’re tied deeply to emotional and neurological patterns—and trying to “correct” them through criticism usually backfires.
Avoid saying:
- “Just stop doing it.”
- “That’s gross.”
- “You’re going to scar yourself forever.”
- “Why don’t you have more self-control?”
These statements only increase shame and can drive the behavior further underground.
Encouraging Recovery With Compassion
Here’s what does help:
- Ask: “How can I support you when you feel the urge?”
- Offer practical help, like finding fidget tools or quiet spaces.
- Acknowledge small victories, like fewer episodes or using coping tools.
- Learn about BFRBs so your support is informed, not judgmental.
Even a simple “I see you’re trying—and I’m proud of you” can be incredibly powerful.
Myths and Misconceptions About BFRBs
It’s More Than Just a Bad Habit
One of the biggest misconceptions is that BFRBs are just “nervous habits” that people could stop if they really wanted to. In reality, BFRBs are compulsive disorders involving neurological differences. Telling someone to “just stop” is like telling someone with asthma to “just breathe.”
These behaviors are hardwired into the brain’s emotional and reward systems and require thoughtful, multi-layered support—not shame.
The Stigma Surrounding BFRBs
Many people with BFRBs are misjudged. They’re labeled as weird, unclean, or mentally unstable—all of which is false and deeply harmful.
This stigma leads to silence, delayed treatment, and worsening symptoms. That’s why open conversations, education, and advocacy are so critical. The more we talk about BFRBs, the more we help those living with them feel seen, validated, and hopeful.
Raising Awareness and Advocacy
Organizations and Resources
There are several incredible organizations working to raise awareness and provide resources for BFRB recovery:
- The TLC Foundation for BFRBs (www.bfrb.org)
- Picking Me Foundation (www.pickingme.org)
- Stop Pulling – Educational campaigns for trichotillomania
These groups offer online support groups, treatment referrals, webinars, toolkits, and more.
You can also find community on platforms like Reddit (e.g., r/trichotillomania, r/BFRBs), Instagram, and TikTok—where lived experiences and recovery content are becoming more visible every day.
Promoting Mental Health Literacy Around BFRBs
Talking openly about BFRBs in schools, workplaces, and media can change lives. Simple actions—like sharing a post, wearing awareness gear, or correcting misinformation—help break the silence and normalize the conversation.
Remember: representation matters. When people see their experiences reflected in others, healing begins.
Conclusion
Body-Focused Repetitive Behaviors are more than habits—they’re signs of deeper emotional needs and neurological patterns. From hair pulling and skin picking to nail biting and cheek chewing, these actions often emerge as ways to self-soothe, cope, or feel a fleeting sense of control.
But they don’t have to define you.
With the right tools, support, and understanding, recovery is not only possible—it’s happening every day. Whether you’re seeking help for the first time or supporting someone who’s struggling, compassion and awareness are the most powerful tools we have.
You’re not alone. And you don’t have to fight this in silence anymore.
FAQs
Are BFRBs a form of OCD?
BFRBs are classified in the same category as OCD (Obsessive-Compulsive and Related Disorders), but they are distinct. OCD involves intrusive thoughts and ritualistic behaviors, while BFRBs involve physical actions that relieve emotional discomfort or sensory tension.
Can children grow out of BFRBs?
Some children may see a reduction in BFRB symptoms over time, especially with support. But many carry the behaviors into adulthood without treatment. Early intervention increases the chance of long-term relief.
Is there a cure for trichotillomania or dermatillomania?
There is no “cure,” but there are highly effective treatments that help people reduce or even stop their behaviors. Many find significant relief through therapy, tools, and lifestyle changes.
How do I know if I have a BFRB or just a nervous habit?
If the behavior causes emotional distress, physical damage, and interferes with daily life, it may be a BFRB. A mental health professional can provide a diagnosis and help determine the best course of action.
What’s the first step toward recovery from a BFRB?
Recognize that it’s a real condition and not your fault. Then, seek support—from a therapist, community, or trusted person. Awareness, education, and compassion are the foundation of every healing journey.