What Are the Depression ICD-10 Codes? The F32 & F33 Guide
Master the nuances of Major Depressive Disorder coding. Learn how to accurately document single vs. recurrent episodes, determine severity, and prevent claim denials.
Major Depressive Disorder (MDD) is one of the most frequently diagnosed conditions in behavioral health, yet it remains one of the most commonly miscoded. When therapists and prescribers rely on generic, "unspecified" codes, they invite insurance audits and risk claim denials.
In the ICD-10 manual, depression codes are heavily stratified by two main factors: episode frequency and severity. Understanding the difference between the F32 (single episode) and F33 (recurrent) code families is essential for ensuring your DAP notes support medical necessity.
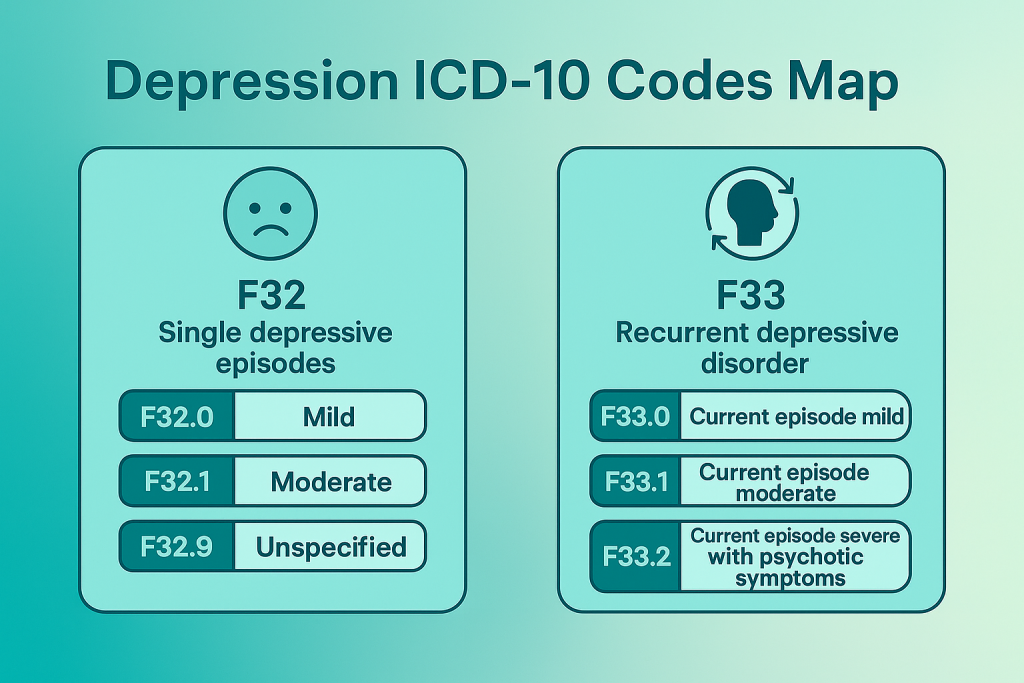
The F32 vs. F33 Distinction
The entire coding structure hinges on whether this is the patient's very first episode of depression, or if they have a history of depressive episodes.
F32 Series: Used exclusively for a patient's first and only Major Depressive Episode.
F33 Series: Used when a patient has a history of at least one previous depressive episode, separated by an interval of at least two consecutive months without significant symptoms.
The F32 Series: Single Episode Depression
If a patient is experiencing their first major depressive episode, you must select from the F32 category. The specific code is determined by the severity of their symptoms, which should ideally be measured using a validated screening tool like the PHQ-9.
| ICD-10 Code | Description | Clinical Indicator / Severity |
|---|---|---|
| F32.0 | Major depressive disorder, single episode, mild | Minor functional impairment; symptoms just meet diagnostic criteria. |
| F32.1 | Major depressive disorder, single episode, moderate | Significant symptoms; obvious difficulties with work, home, or social activities. |
| F32.2 | Major depressive disorder, single episode, severe without psychotic features | Considerable distress; marked interference with daily functioning; active suicidal ideation may be present. |
| F32.3 | Major depressive disorder, single episode, severe with psychotic features | Severe depression accompanied by hallucinations or delusions. |
| F32.4 | Major depressive disorder, single episode, in partial remission | Full criteria no longer met, but some symptoms linger. |
| F32.5 | Major depressive disorder, single episode, in full remission | No significant symptoms for the past 2 months. |
| F32.89 | Other specified depressive episodes | Symptoms do not neatly fit standard criteria, but clinical depression is present. |
| F32.9 | Major depressive disorder, single episode, unspecified | Use sparingly. Payer scrutiny is high for unspecified codes. |
| F32.A | Depression, unspecified | A general code when a more specific diagnosis cannot be made (e.g., brief intake screening). |
The F33 Series: Recurrent Episode Depression
Once a patient experiences a second distinct depressive episode, their diagnosis permanently shifts to the F33 category. You will no longer use F32 codes for this patient, even if years have passed since their last episode.
Coding Recurrent Depression
The F33 subcodes mirror the severity structure of the F32 series:
- F33.0 — Recurrent, mild
- F33.1 — Recurrent, moderate
- F33.2 — Recurrent, severe without psychotic features
- F33.3 — Recurrent, severe with psychotic symptoms
- F33.41 — Recurrent, in partial remission
- F33.42 — Recurrent, in full remission
3 Steps to Accurate Depression Coding
Assess Severity
Use clinical tools like the PHQ-9 to establish and document mild, moderate, or severe baselines in your intake.
Check History
Thoroughly screen for past episodes to determine if the diagnosis is a single episode (F32) or recurrent (F33).
Note Psychosis
Explicitly document the presence or absence of psychotic features, as this dramatically shifts the code selection.
Common Coding Mistakes and Denials
Payers are increasingly rejecting claims that rely on lazy coding habits. To protect your revenue cycle and ensure compliance, avoid these frequent errors:
- Overusing F32.9 or F32.A: Relying on "unspecified" codes indefinitely signals to insurance companies that you have not properly evaluated the patient. Unspecified codes should generally only be used during the initial evaluation phase.
- Failing to code co-occurring conditions: If the patient also suffers from panic attacks or OCD, ensure you are utilizing the correct Anxiety ICD-10 codes alongside the F32/F33 code to capture the full clinical picture.
- Mismatched CPT Codes: If you code a "severe" depression episode (F32.2) but only bill a low-level E/M code like 99203 without a psychotherapy add-on, auditors may question why the treatment intensity does not match the diagnostic severity.
- Missing documentation: The severity level you select (mild, moderate, severe) must be explicitly justified in the narrative of your SOAP notes.
Stop Guessing on Medical Codes.
Start Getting Paid.
- Professional Medical Coding & Billing
- Denial Management & Appeals
- FREE Insurance Credentialing
- FREE TherapyDial Profile Listing
We verify your ICD/CPT pairings, submit your claims, and fight for your revenue.
HIPAA Compliant & Expertly Managed.
Frequently Asked Questions
TherapyDial Editorial Team
This article was reviewed and updated by the TherapyDial Clinical Revenue Team. Our content follows strict guidelines to ensure coding accuracy, relevance, and compliance. We monitor ICD updates to provide mental health professionals with the most reliable operational information.